by Sarah Apple Kingsley, pt, dpt
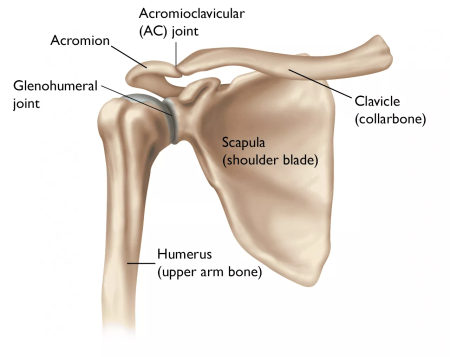
When most people think of shoulder pain, weakness, and dysfunction, their next thought is rarely if ever, “well what about pelvic posture?” In most health care and physical therapy settings, the scope of treatment is very narrowly focussed on the primary issue or problem at hand. An orthopedist or medical doctor may choose to inject a cortisone shot to the area or request an MRI to diagnose a rotator cuff tear or issue. A typical physical therapist in this scenario would likely prescribe some shoulder stretches and multiple shoulder strengthening exercises. If they are a good therapist, these exercises will hopefully include those to help strengthen the scapular stabilizing muscles.
Unfortunately, even in this “best case PT” scenario, it is still possible to miss the broader picture. Studies and evidence have shown that many of the standard treatment exercises, when performed in isolation, can be ineffective in resolving or even improving shoulder pain, weakness, and dysfunction. So why is that? A GREAT PT needs to look at the whole body and how each segment relates, connects, integrates, and participates with each other for true working order. At the center of this multifaceted working vessel is…..THE PELVIS!
Spinal posture plays a large role in the strength and function of the shoulder. Consider, for example, a patient with weak shoulder strength and limited mobility. When the patient’s pelvis is anteriorly tilted, or tipped forwards, this creates an increase in lumbar lordosis. We are supposed to have a natural small arch in our low back, but the excessive curve or “swayback” as it is commonly termed is due to an anteriorly tilted pelvis. This increase in lumbar LORDOSIS directly relates to an increase in thoracic KYPHOSIS. An increase in thoracic kyphosis or rounding/humpback of the upper back contributes to an anteriorly tilted and internally rotated scapula, which causes the rounded shoulder posture. EMG studies have shown that this forward shoulder posture limits the activation of the scapular upward rotators such as your upper and lower trapezius as well as significantly reducing the firing of the serratus anterior muscle, our major scapular stabilizer. Less activation = less strength = less function!
With typical shoulder dysfunction, we tend to see an OVERactivation of the upper trapezius muscle. This leads to excessive shoulder hiking, causing pain and strain in the neck and shoulders due to a compression of the nerves, muscles, and ligaments in the subacromial space and often leads to rotator cuff tears or thoracic outlet syndrome. Conversely, a well-working shoulder primarily uses what is referred to as the “forced couple” of each the upper and lower trapezius as well as the serratus anterior to aid in the initial upward rotation of the shoulder to work effectively and prevent strain, compression, and injury when reaching up overhead. A forced couple is when two muscles with opposing actions work together with equal forces in order to create one action simultaneously, in this case, upward rotation of the scapula.
EMG assessments can specifically show that an increased anterior pelvic tilt increases the activation of the upper trapezius and decreases the work of the lower trapezius and serratus anterior. When pelvic tilt was reduced, the results showed a significant INCREASE in the activation of both the lower trapezius and serratus anterior, while just slightly decreasing the activity of the upper trapezius. When just the upper trapezius is active or overactive, this typically leads to more pain and dysfunction and less range of motion. With more equal activation of all 3 supporting muscles, the joint can function more optimally, with more strength, more range of motion, and less pain and injury!
So how can we promote better activation, strength, AND function of the shoulder complex??!! Neutralize the pelvis! Reducing the anterior pelvic tilt posture can have dramatic changes on the working order of the shoulder girdle. How do we do this? Our LYT yoga classes are amazing at retraining the body how to properly stack the girdles of the shoulders over the pelvis and hips. This not only provides the best stability but also the best functional strength and adaptability for powerful and reactive movement through a variety of planes of motion.
If you are anteriorly tipped in the pelvis it is likely that your hip flexors (the muscles in the front of your hips) are tight and also possibly weak, but even more likely that your gluteals and hamstrings (the opposing muscles) are very weak. Working the strength of these posterior chain muscles by biasing a POSTERIOR pelvic tilt or slight tucking of your tailbone can help reduce this excessive arching of the low back. We also stretch the hip flexors in each of our LYT yoga classes by coming into a 90/90 low lunge position. It is important to focus on keeping the back knee directly underneath the hip, wrapping the back glute under, and lifting up in the abdominals to create an active stretch into the front hip muscles, as opposed to leaning forwards which creates additional compression into the hip joint structures and also likely further biases an already anteriorly tilted pelvis position.
References: