by Michelle F. Onion, PT, MSPT
Why is talking about the pelvis so important? Because it is our base, our center. Our trunk “rests” on it and our legs come out from it. When it is not in an ideal position it can impact how we move and the ease with which we move.
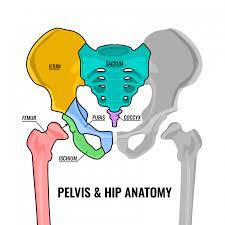
Let’s first talk about the bones of the pelvis. The largest bones are the ilium. There are two, one on each side. In the back, the ilium attaches to the sacrum. As the pelvis comes around you have the pubis bones on the top and they attach at the front at the pubic symphysis. At the bottom, the ischium attaches to the pubis and creates the obturator foramen (the large hole that sits between the bones). The ischium is angled lateral and anterior. It, in conjunction with the ilium and pubis, forms the acetabulum (hip joint). The inferior or posterior position of this acetabulum is determined by a posterior or anterior pelvic tilt, but there is a slight inferior orientation to it in neutral. The ilium, ischium, and pubis move as one but remember there are two sides. They can move in and out relative to neutral, rotate forward and backward, and slide up or down. This is a slight movement but movement nonetheless, that can impact muscular function altering both ease of motion and which muscles do the primary work.
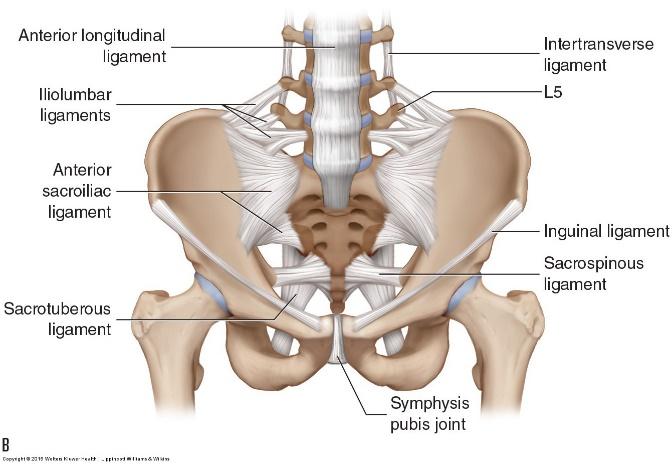
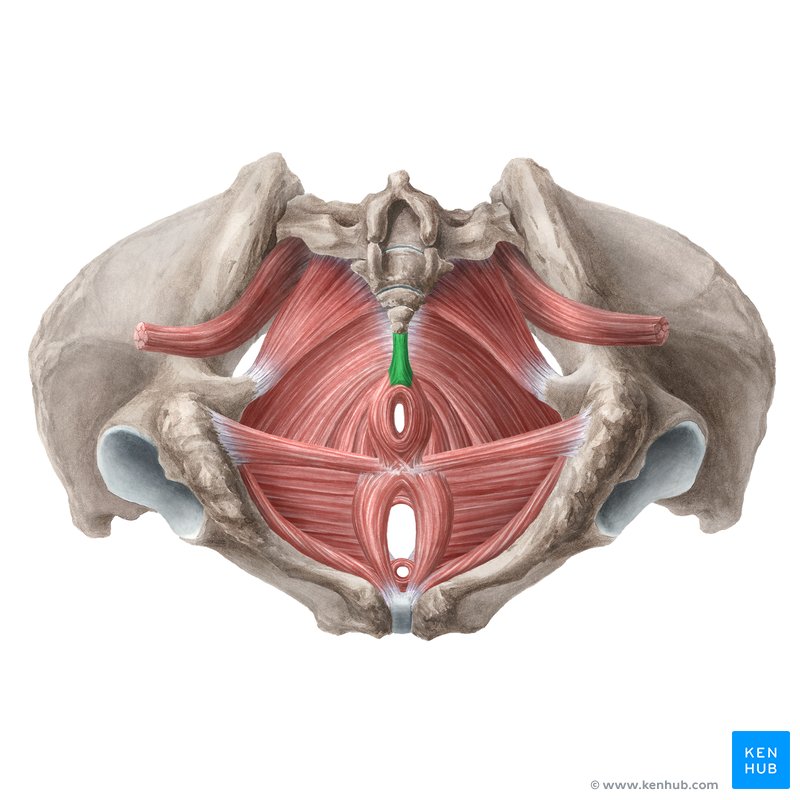
There are multiple ligaments in the pelvis, spine, and hips that help to control and support. They are our enforcers. Bones are not stable in and of themselves but work in conjunction with muscles and ligaments to create stability.
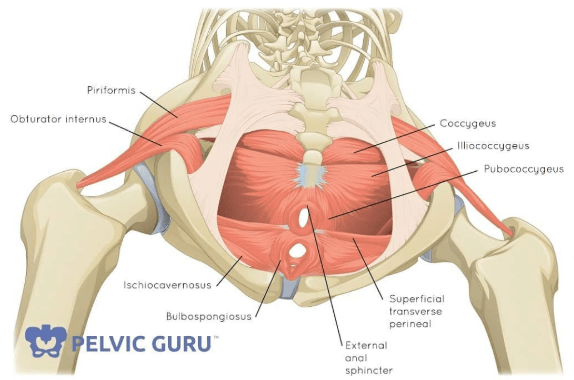
Notice how the muscles and ligaments fill in the foramen (holes) of the pelvis. They act as a sling to support all that sits in the pelvic and abdominal cavities. They are a support system and they are crucial in keeping everything contained. This is our pelvic floor.
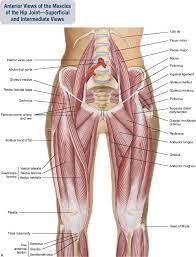

What I want you to notice from these two pictures of the muscles is how the pelvis connects the lower body, trunk and ultimately the upper body. Here you have the muscular connections. You can start to get an appreciation of how movement in the legs impacts what happens in the abdominals, glutes and vice versa. Small movements within the pelvis can allow the muscles in each of these regions to operate optimally or suboptimally.
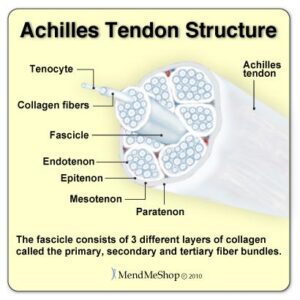
And then we have the addition of fascia. Fascia is the support structure that has just recently been given more attention. Think of fascia like plastic wrap. There is a strength and pliability to it. If you take a piece of plastic wrap and pull at one end of it, there is a far-reaching ripple effect impacting the entire piece of wrap. And fascia is everywhere and a big connecter of the lower and upper body. Small nuances in the pelvis can impact how the fascia moves. If it pulls or if it is more fluid, if it allows or prohibits movement.
Let’s think about how this applies to yoga and our daily lives. If the pelvis lives in an anterior or posterior pelvic tilt, muscles will be at a disadvantage and unable to work as well for you or for your clients. Our core will not be able to engage fully. Our glutes will snooze even more. Our pelvic floor will have difficulty supporting all that depends on it for structure. And this has a huge impact on our movement and functional capabilities.
If you look at the lower body. Our femurs will not be able to move well in the acetabulum (hip joint) and we will potentially have impingement and pain changing our movement patterns even more. As our hips move in this altered manner it impacts the ability for our knees to function which, in turn, impacts what our feet do. It is a complementary system. You lose optimal movement in one area and the other areas are impacted. We will lose the possibility of overall optimal movement.
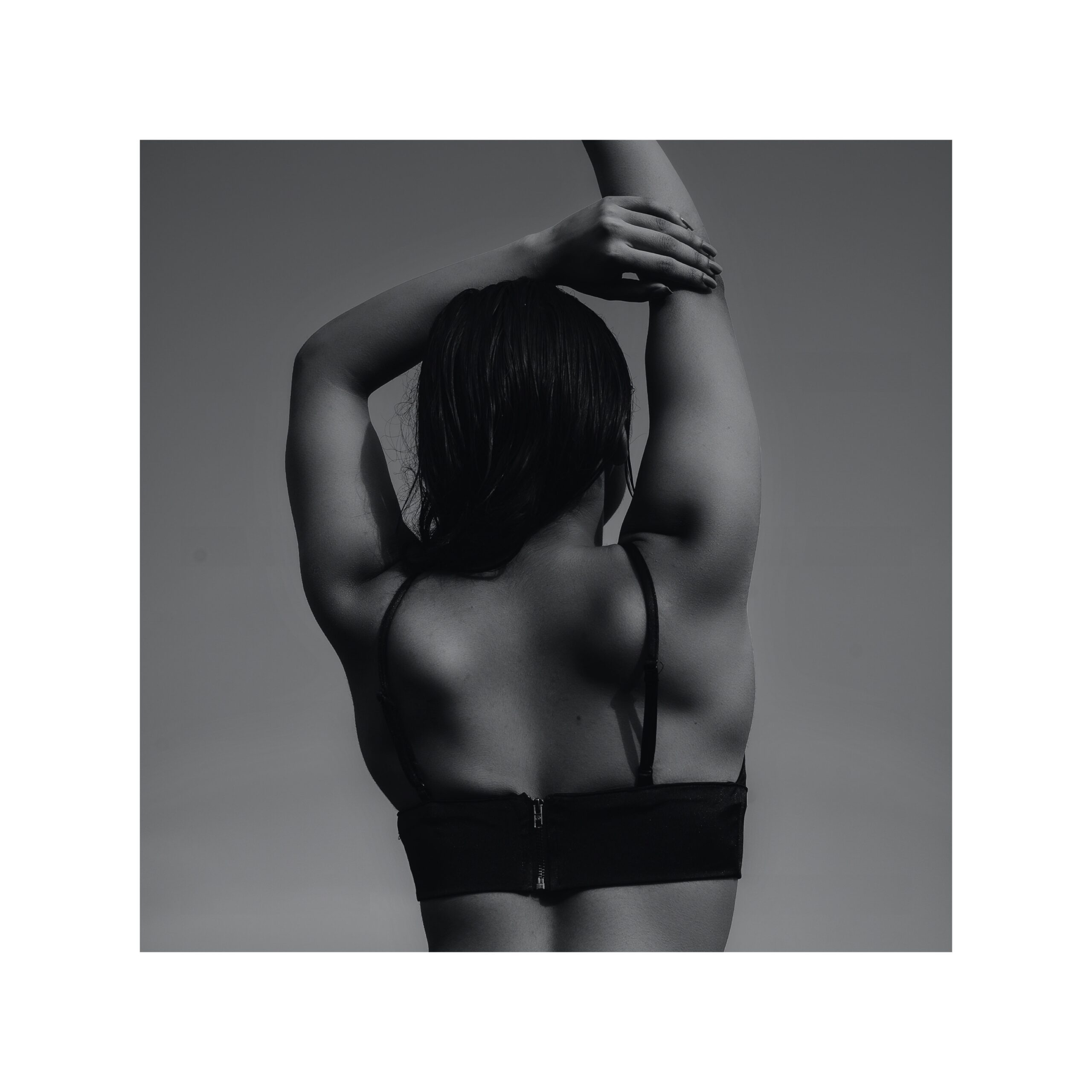
Looking at the upper body. The structure and position of the trunk impacts the pull on the scapula impacting the stability and mobility of how the scapula move with shoulder motion. The scapula and humerus have a rhythm that allows for or takes away from good movement patterning. The difference with the upper extremity and lower extremity is that the upper extremity is not fixed to the ground so the impact on the elbow, wrist and hand may not be as noticeable, but there is still an impact.
And this all comes from our center, our pelvis. It is why LYT focuses on a neutral pelvis, not to make things difficult, but to allow our body to have access to optimal movement patterns. To be dynamic in our everyday. If your clients have difficulty with finding neutral, think about the other ways a pelvis may move: in/out; up or down. There might be a dysfunction there and physical therapy may address this. Perhaps helped with a joint mobilization or muscle energy technique that a PT can perform. And then the neutrality can be supported through our practice of LYT.
As you take time to consider the pelvis, think about how this impacts your individual function. Get to know its impact on your own movement, on your own function, and take this exploration to your clients and to others around you. We have the gift of guiding others through their own exploration of their individual movement. Helping others find their center, their base. Creating structure to allow for more optimal, dynamic movement. Enjoy the exploration!