by Ashley Newton, PT, DPT
Pelvic floor strength is more than just the ability to squeeze the muscles while waiting in line for the bathroom. Pelvic floor muscle functioning is about a muscle’s ability to adapt and the amount of muscle activity it is able to generate and coordinate. So let’s dive into pelvic floor muscle functioning and adaptability in pelvic floor strength and overall pelvic health.
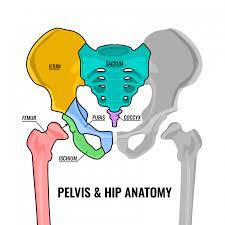
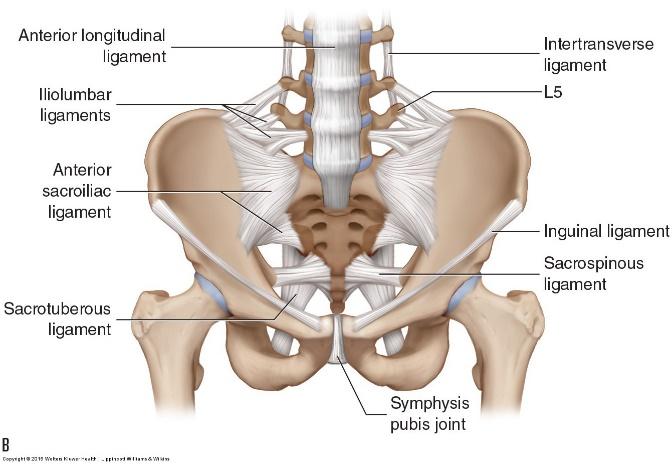
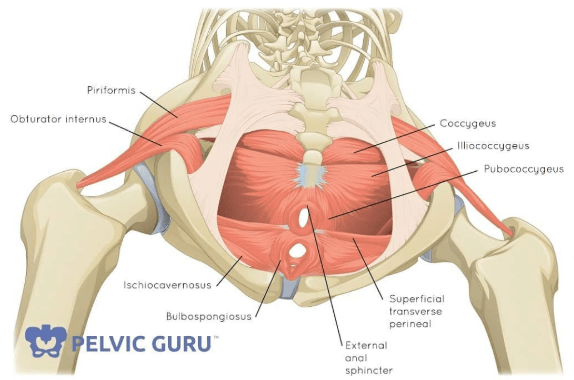
Let’s start with this myth-buster: pelvic floor muscle tightness does not equal strength! The pelvic floor consists of three layers of musculature and a layer of endopelvic fascia. The pelvic floor muscle actions include 1) contraction, 2) relaxation, and 3) lengthening. For optimal functioning, the pelvic floor needs to be able to coordinate these three movements to support our posture, support the organs above, and provide stability to the pelvic bones. If a muscle is tight – meaning it is not able to move through its full range of motion (able to contract, relax, and lengthen) completely, it is not able to do its job to the best of its ability. Think about it this way – if you made a fist with your hand and repetitively squeezed it and then tried to write a 1,000-word essay, your hand may feel sore and tired, making it difficult to write that essay. Similarly, if the pelvic floor is squeezing, contracting all the time and then it comes time for it to work on stabilizing/supporting, it will have trouble doing this job effectively. So, when it comes to pelvic floor strength, tightness and tension can actually mean weakness. For optimal pelvic floor strength, the pelvic floor needs to be adaptable and be able to shift between contraction, relaxation, and lengthening when appropriate.
So, when should the pelvic floor be relaxing fully? How about lengthening? Pelvic floor relaxation occurs when we breathe. On the inhalation phase of a breath, the pelvic floor descends/relaxes. Now when we are moving and exercising we may not be as consciously aware of this change in muscle activity because the pelvic floor needs to maintain some contractile activity to support the trunk in space. When you are in savasana, however, which is a position where your body is fully supported, the pelvic floor will relax further than when exercising. The feeling of pelvic floor relaxation is a downward movement (down toward the toes) of the tissues between the SIT bones. It is not a grand excursion, meaning it is not as obvious as contracting and relaxing your bicep muscle, but should feel like a gentle stretch downward. Now just because someone has difficulty differentiating between whether the pelvic floor is relaxing vs. contracting does not mean it is not happening. When we start talking about and giving more attention to these muscles, our brain adapts and devotes more attention and brain space to focusing on the sensations there. Thus, the more we consciously think about pelvic floor movement, the better we get at differentiating pelvic floor contraction vs. relaxation.
Lastly, what is lengthening?! This one may be the most difficult to feel as we do not often consciously practice this technique. And to be clear – when speaking to pelvic floor lengthening, I am speaking to an eccentric pelvic floor contraction. Let’s go back to the metaphor of the hand. If making a fist is contracting, opening the hand is relaxing, and stretching the fingers wide would be lengthening/eccentric contraction. Pelvic floor relaxation is the period where the pelvic floor muscles stop contracting during lengthening, the muscle fibers are still contracting but in the downward direction. We most often use this type of contraction with voiding strategies and even with pushing during labor/delivery of a child.
Ultimately, pelvic floor strength is more than just a muscle’s ability to shorten/squeeze (it’s more than just Kegels!!). It is its ability to be adaptable: to lengthen, relax when appropriate, and shorten enough to stabilize and support. Simply squeezing the pelvic floor and expecting it to do its job when we jump, practice yoga, and transition between postures is not realistic. Get in tune with the muscles of the pelvic floor and see if you can contract, relax, and lengthen the musculature. If not, and you have issues such as pain, urinary leakage, constipation, and/or scarring, it may be useful to contact a pelvic floor physical therapist to assess the pelvic floor and its relationship to movement so that you can move optimally!
<3 Ashley
@ashleynewton_dpt