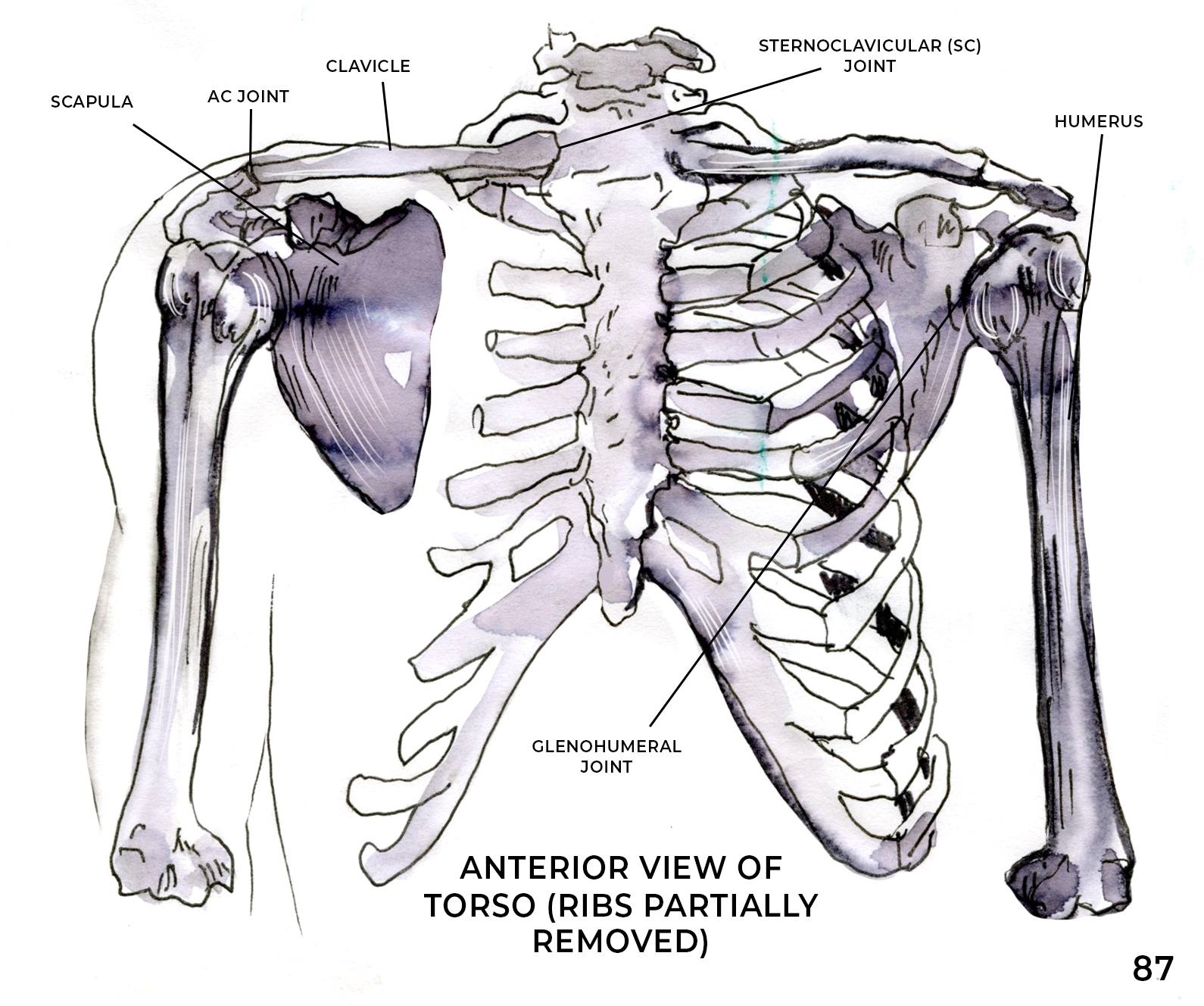
When most people think of the shoulder joint, they usually only consider the space where the ball of the upper arm bone (humerus) articulates with the socket of the shoulder blade (scapula). In fact, most people don’t even know the socket is part of the scapula. Furthermore, calling the shoulder a “ball and socket” joint is a stretch, as it’s really more like a golf ball sitting on a tee. The socket is actually a small shallow disc (glenoid fossa). The ball (humeral head) is held in place passively by ligaments of the joint capsule and actively by the muscles of the rotator cuff. But the shoulder itself is really more of a “complex”, consisting of four separate joints that must work together to keep the shoulder complex functioning properly:
- Glenohumeral Joint – Humerus and Scapula
- Acromioclavicular Joint – Scapula and Clavicle (collar bone)
- Sternoclavicular Joint – Sternum (breast bone) and Clavicle
- Scapulothoracic Joint – Scapula and Rib Cage
Unlike most joints of the body in which two bones are connected by ligaments and/or discs, the scapulothoracic joint relies purely on a coordinated dance of 17 muscles that attach to the scapula, as well as the mobility of the other three joints, to provide stability for the rest of the arm and shoulder. SEVENTEEN MUSCLES!!! Weakness in any one of the muscles attaching to the scapula, but particularly the large ones like the serratus anterior (Lara’s favorite!), latissimus dorsi, trapezius, and rhomboids, can affect how the shoulder and ultimately the entire upper extremity moves and functions. Poor movement patterns, muscular weakness, and limited joint mobility can lead to pain in and injury to the neck, shoulder, spine, elbow, wrist, and hand.
Whether you are playing a racquet sport, doing yoga, or just trying to put away the dishes in an overhead cabinet, scapular strength and mobility are key to preventing injury. Weakness in these large “core” muscles can lead to overuse of the smaller muscles of the upper extremity and thereby cause injuries.
The muscles of the scapula form force couples, which are muscular co-contractions that properly position the scapula for maximum shoulder function and provide a stable base of support for the entire upper extremity. It has been estimated that throughout 90% of shoulder range of motion, muscles (and not passive structures) are responsible for shoulder stability. Scapular issues are commonly seen in people with tight and overactive upper trapezius and pectoralis minor muscles, coupled with weak/underactive lower trapezius and serratus anterior muscles. This decreases the ability of these force couples to occur, resulting in decreased static and dynamic positioning (stability) of the scapula during movement.
Corrective exercises can be very successful in restoring neuromuscular control of the scapula, helping to return to normal function and enhancing the overall function of the shoulder complex. An exercise program should include proximal kinetic chain exercises aimed at improving scapular muscle strength, flexibility exercises to minimize tight muscles pulling the scapula out of position, and exercises to enhance these functional force couples. In Lara’s podcast, Redefining Yoga, Episode 269 Wednesday Q & A, she describes some great ways to improve your scapular strength and stability. We will also be featuring some classes focused on the scapula in this week’s upcoming LYT® Daily, so be sure to check it out! One of the best places to begin to strengthen and stabilize the scapula is on your mat. I look forward to seeing you there!
Xoxo,
Kristin

