When my kids were little and needed to be soothed, I would have them lie across my lap and I would count their bones. I’d tell them what each bone was called by their full Latin name and eventually move onto the muscles. They LOVED it. I’ll never forget the first time Betsy fell down and told me that she “scraped her patella”! I was at first super proud and then a little horrified, imagining the hard time the kids in her class would give her for being weird or the looks I’d receive from the school teachers! Luckily, they quickly outgrew the medical terminology, latched onto the easier terms like “kneecap” and “elbow” (instead of olecranon process), and any social trauma I might have inadvertently caused was averted. 🙂
As we grow older, whether or not we choose to go into medicine, pretty much everyone learns that the kneecap is called the patella. So many people experience knee pain at one time or another, or know someone who has, making terms like patellofemoral syndrome and patellar tendinitis commonplace. Since I’ve gotten back into regular jogging, my patellae are making themselves known again. Sometimes I’m afraid you all can hear the crackling over Zoom when I come from a deep squat to stand! Why does that happen? What is that noise? What is the point of the patella anyway? I hope to answer all three of those questions and if you’re interested in the answers, read on.
The patella is also known as the kneecap. It’s the largest sesamoid bone in our body. Sesamoid bones are bones embedded within a tendon or muscle. It attaches the tendon of the quadriceps to the tibia, via the patellar ligament. The patellar ligament is also known as the patellar tendon, but since it goes from the patella (bone) to the tibia (bone), it’s technically called the patellar ligament.
The primary function of the patella is to act as a fulcrum for the quadriceps, increasing its extensor strength by 33-55%. The bottom surface is covered by 3-5mm of cartilage, which is the thickest layer of cartilage anywhere in the body. The structure of the knee joint is such that the compressive force on the patella is SEVEN times the body weight when descending stairs, so it’s no wonder its articular cartilage is so thick! However, it should come as no surprise that it is subject to wear and tear over time with repetitive climbing, descending, and running on hard surfaces. Under normal circumstances, the role of the cartilage lining the undersurface of the patella is to decrease friction between the patella and the groove of the femur, in which it articulates. Sometimes we have issues that arise with the “tracking” of the patella within this groove and we develop areas of increased wear, called crepitus. The crackling sound from the knees when going from squat to stand or vice versa is secondary to crepitus. The smooth surface of cartilage is normally soundless. When we start hearing noises (aka crepitus), it’s because the surfaces are no longer smooth…more like sandpaper.
There are several different reasons why the patella may not track correctly, including:
- Weak hip muscles – poor gluteus medius strength allowing internal rotation of the femur and “knocking” on the knees
- Poor static alignment of the patella – too high or low, tilted, or rotated
- Connective tissue restrictions around the patella – too tight or too lax
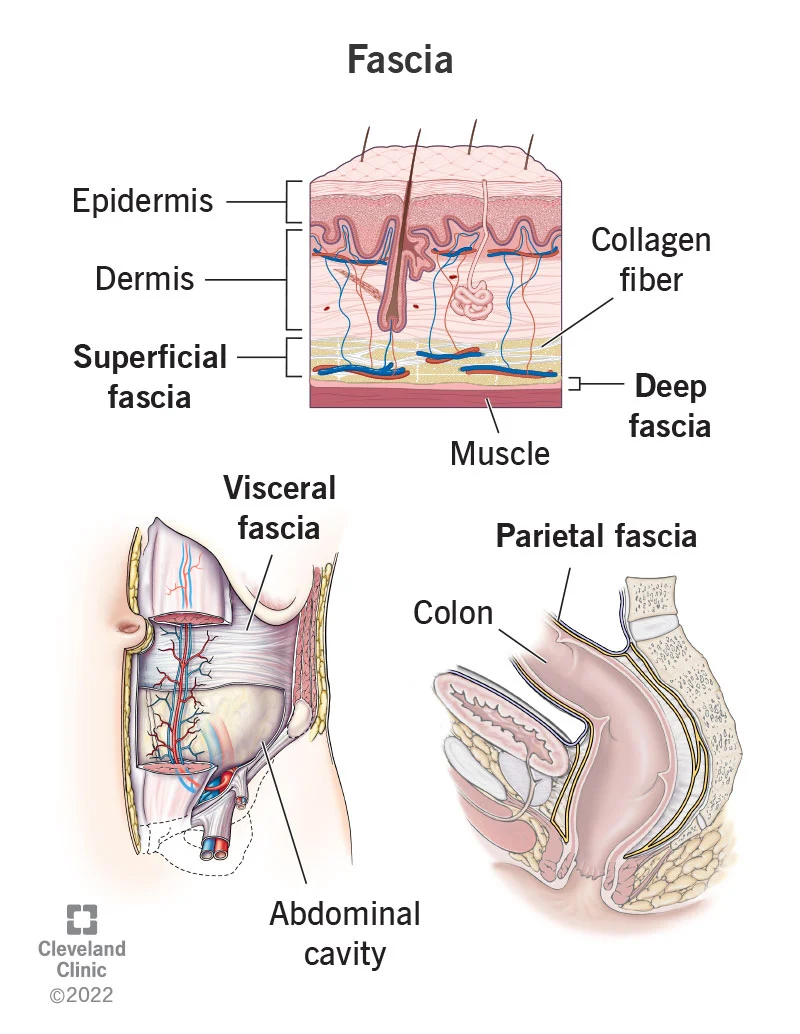
We can have the greatest effect on patellar tracking with movement retraining. Strengthening the hips, glutes, hamstrings, and core musculature. The knee joint really just wants to flex and extend, keeping the patella tracking superiorly and inferiorly. Keeping the knees moving over the feet allows for this. Not allowing the knees to go over the toes with repetitive up-and-down movement is also ideal. Keeping our body weight within normal limits, without any added body weight pressure on the patella is crucial. Mobilizing the soft tissue structures surrounding the knee, including both fascia and muscles, to allow the patella to track freely up and down is a great way to minimize patellofemoral wear and tear.
Keep on track with your LYT yoga practice, which challenges the body and core in all of the above ways! https://old.lytyoga.com/
See you on the mat!
Xoxo,
Kristin