Many of you who practice with me regularly know that I have a cranky right shoulder. Several years ago, I was working on a fellow physical therapist who is around 6’2” and roughly 250 lbs. His back was bothering him so I wanted to help him out. It had been a long morning of treating patients. I began to manipulate his sacroiliac joint, a maneuver that requires me to thread my arm through his. In this maneuver, my right shoulder was flexed and internally rotated.
I’ve done this technique thousands of times without any issue, but this time when I leaned away and used my body weight to roll him, I felt and heard a tearing in my shoulder. He heard it too. He looked at me, I looked at him, and we simultaneously muttered, “Uh-oh.” I never had any diagnostic tests done and rehabbed it myself, but I suspect I tore my labrum.
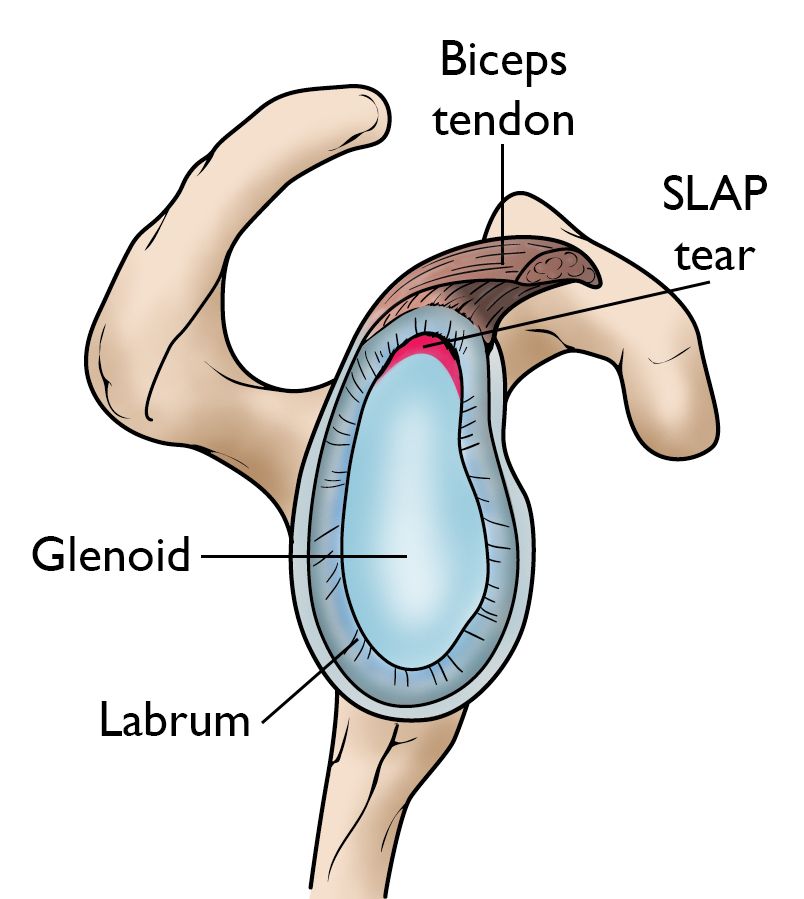
The labrum of the shoulder is a fibrocartilaginous rubbery rim attached around the margin of the socket. It cushions the joint called the glenoid fossa, which is part of the scapula (shoulder blade). The socket is quite shallow and small, covering at most only a third of the ball (the head of the humerus).
One function of the labrum is to deepen the socket. It increases the contact area between the ball and socket by 2 mm at the front and back and 4.5 mm at the top and bottom. If you took a cross-section of the labrum, it would look like a triangle, where the wide base attaches to the edge of the socket, leaving the edge of the labrum thin and sharp at the point. This shape allows it to almost act like a washer, sealing the ball and socket together.
This is called a “viscoelastic piston effect” and maintains a negative pressure within the joint. It’s especially effective against traction or pulling stresses and, to a lesser extent, against shearing stresses. Finally, the labrum provides an insertion point for stabilizing structures, including the joint capsule ligaments and the tendon of the long head of the bicep muscle.
The labrum is often compared to the face of a clock, with 12 o’clock being at the top (superior), 3 o’clock at the front (anterior), 6 o’clock at the bottom (inferior), and 9 o’clock at the back (posterior). Most instabilities in the shoulder are associated with injuries to or changes within the glenoid labrum, particularly where the long head of the biceps tendon inserts at the superior (12 o’clock) portion. They are commonly called SLAP tears, as they involve a Superior Lesion from Anterior to Posterior, usually between 10 and 2 o’clock.
Different types of SLAP tears typically involve different mechanisms of injury. A common mechanism is falling on an outstretched arm or pulling suddenly when lifting a heavy object, as I did with my fellow PT. Other mechanisms include repetitive shoulder abduction and external rotation, like the movements that many throwers, overhead athletes, or manual laborers perform over and over. A direct blow to the shoulder, as with tackling in football can also be a cause. SLAP tears can occur in a degenerative manner for the aging population as well.
Treatment for SLAP tears includes both nonoperative and operative measures. Both have proven successful among certain populations. Previous studies indicate that nonoperative management is successful for anywhere from 22 to 85% of patients. Operative repair in adults is reported to be successful for between 80 and 97% of patients. It often helps alleviate the pain and return of range of motion.
Among overhead athletes, many patients are unable to return to their prior level of performance. Results vary widely in this population, with between 7 and 84% demonstrating a return to their prior level of performance. As patients age beyond 40 years old, surgeons typically opt to perform a biceps tenodesis. In this surgical procedure, the tendon of the long head of the bicep is detached from the labrum and anchored to the proximal humerus. Repair success rates are lower among older populations, so this is the most effective treatment of choice.
I continue to address my shoulder issue with home exercises and activity modifications and so far, so good! As I say all the time in Stretch class, the shoulder joint is our most mobile, but also our most unstable. For all the parts to work in harmony, it requires a high quality of movement. Paying attention to how we move on our mats and keeping the ball centered in the socket is important for many reasons, but especially to avoid placing repetitive undue strain on the labrum.
Continue using your LYT Yoga® practice to build strength and good brain mapping in the shoulder joint complex. Until then, I’ll see you on the mat!
Xoxo,
Kristin