by Kaitlin Acharya
How to Adapt Your Yoga or Movement Practice for Pregnancy: Second Trimester
Enjoy the extra energy, mindfully
Welcome to my favorite trimester. Hopefully, by now many of the difficult first trimester symptoms have subsided and you feel a surge of energy. In my experience, it was more of a return to feeling like my usual self, which did mean more energy compared to the first trimester. If you toned down intensity during the first trimester because of fatigue, you may feel like you can turn things back up now, but don’t go too hard. Listening to your body is still very important.
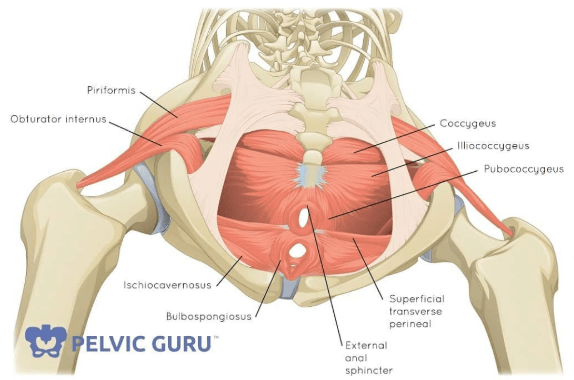
Continue to work on connection to your core, but you will want to start modifying to avoid any movements where you cannot control the pressure within your abdominal cavity (also known as intra-abdominal pressure, or IAP). Pay attention to any soreness in the pelvic region or low back which can be indicators that you are pushing the intensity too hard and over-stressing your pelvic floor and core. Overhead movements, like pull-ups or shoulder press, can overload the ever-stretching abdominals at this point so keep an eye on your belly if performing these movements. Jumping and high-intensity cardio can have negative effects on joints and the pelvic floor so it’s a good idea to start modifying these types of movements as well. Crunches and sit-ups are also not advised, but that doesn’t mean you can’t work on core connection while lying on your back. Supine breathwork is a great way to connect to your pelvic floor and core without over-stressing the abdominals. It’s also a great way to train your focus for labor. Again, check out my blog post on this type of breathing.

Mind the growing bump
As your baby grows, so does your belly and you’ll start to show at some point this trimester depending on your body and whether you’ve had a baby before. Especially on the yoga mat, you will need to start modifying movements to accommodate the bump. Any position where you are lying on your belly may start to become uncomfortable, like cobra and locust. At this point, move to all fours and practice a similar movement like cat-cow or bird-dogs.
Blocks are going to be your best friend. Use them to modify plank, down dog, and forward folds. They are also great for creating space around the belly in any sort of pose where you are bent over and have one or both hands on the floor – like fingertip lunge or side lunge. You can also widen your stance in any pose to create more space for the belly. Play around with the height of the blocks to find a position that is comfortable for you. This is also the time to be mindful of twisting. Gentle twists in the thoracic spine are ok but do not force the twist – something I don’t recommend to even my non-pregnant students. Placing a hand on the belly for abdominal support and to monitor any unmanaged IAP is also helpful. And of course, if they just don’t feel good, don’t do them!
Mindset matters
I realize much of this post is focused on what you can’t do or may have to limit as a pregnant person, but know that there is still so much that your body can do during this time! Personally, I felt myself being amazed and appreciative that my body was still able to move on my mat and lift weights all while growing a human inside of me. Sure, some poses looked a little different, I wasn’t doing any of my beloved handstands, and I had lowered my weights a bit but I was still moving and breathing and taking time to focus on myself and my body. Pregnancy is temporary. It may not feel that way by the time 36 weeks rolls around (me currently: have I been pregnant for 9 months or 9 years?!), but you will have your baby and with proper post-natal care you will be able to return to your regular movement practice.

How to Adapt Your Yoga or Movement Practice for Pregnancy: Third Trimester
The Final Countdown
The last trimester – you’re almost there! This trimester can be fraught with discomfort as the belly grows even bigger and muscles and ligaments loosen even more thanks to that relaxin hormone. Fortunately, movement can help lessen pain and prepare for you for labor and delivery.
Lighten the Load
I like to think of movement intensity during pregnancy like a bell curve. You may lack energy during the first trimester, but slowly start to regain it and peak during second trimester. Then third trimester comes around and the body needs less of that intensity to prepare for birth. This doesn’t mean you should cease all movement, but as I advise throughout this series, listen to your body. Mine was screaming at me to slow down practically on the day that I hit the third trimester. My low back started hurting, walking up stairs left me a little winded, and even bending over was getting difficult. So I modified even more. At this point in my pregnancy my yoga practice was heavily modified, focused on connecting with my breath and staying mobile in my hips to help with labor. I was still getting my heart rate up during my weightlifting workouts, although weights were extremely light.
Modify Daily Movements
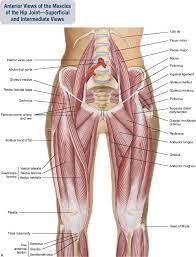
In addition to continuing to modify your movement practice as you did in the second trimester, it’s also important to consider modifying movements outside of your exercise regimen or yoga mat. If you haven’t already, start modifying how you sit up, whether from laying down on your mat, the sofa, or your bed. It’s best to roll to your side first and use more of your obliques to sit up so that you are not over-stressing the already stretched and stressed rectus and transverse abdominus muscles, as well as the linea alba, the midline connective tissue that holds your abdominals together.
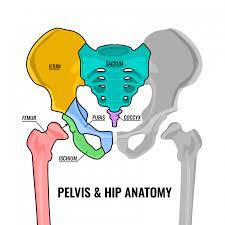
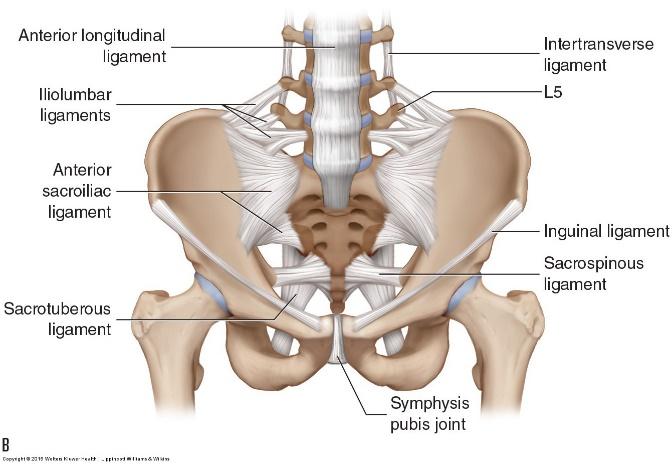
Bending over may also have become more difficult. Try widening your stance, squatting instead of hinging at the hips to pick something up (bending more in the knees and lowering the butt towards the ground), and sitting down to put your shoes on…maybe even enlisting your partner or a friend to help with that last task 😆. Balancing can also become noticeably difficult during this trimester and maybe even painful in the pelvic area due to separation of the pubic symphysis or issues with the SI joint.* You can ease this pain by avoiding unilateral positions (anything that uses only one leg) or shortening your stance.
*among other possibilities — the pelvis has a lot of muscles and ligaments attached to it! But these are most common in pregnancy.

Movements to Help with Labor
Every mama wants to know how to ease the arduous task of birthing a baby — I mean, who wouldn’t?! Here are some movements that can help prepare your body for labor.
- Down Dog – Downward-facing dog is actually classified as an inversion since your head is below your heart in this pose and it is a great position to help relieve stress on the pelvis and even move the baby out of the pelvic outlet for repositioning. If your baby is in a breech position, this pose can help, but I also suggest checking out Spinning Babies and the Webster Technique for more professional help with getting the baby in a head-down position.
- Cat/Cow with knees together, feet wide – This was one of my go-to movements in my third trimester. Keeping the knees together and feet wide internally rotates the hips and creates more space in the back of the pelvis, which at this point in pregnancy is probably holding a lot of tension from the load of the baby in front.
- Squats, squats, and more squats – Squats are fantastic for opening the pelvis and preparing the perineum for childbirth. There are so many different varieties as well – goddess squat (legs wide, feet turned out), asymmetrical (one foot on a higher surface), the LYT happy squat (hips high, head down, arms forward – great for the low back), side lunges, and more.
One Last Thing…
My most important recommendation for labor – don’t forget to BREATHE!! Keep practicing that 360 degree-breath all the way through labor and beyond. It is truly going to be your best tool.
Happy and healthy birthing!
by LYT teacher Kaitlin Acharya
Website: www.yogakaitlin.com
Instagram: @yogakaitlin